Comprehensive Audiological Evaluations:
 Otoscopic Evaluation: This test is simply to check the ear canal. We evaluate the ear canal, structures of the ear canal and look for abnormalities (tumors, growths, etc.), wax, fluid, excessive ear hair, we assess the anatomy of the ear canal (narrow, closed, etc.), and evaluate the status of the eardrum. We look at the eardrum color, (red, white, yellow) the translucency (transparent, opaque) and position (retracted, neutral or bulging) of the drum. Look for scarring of the eardrum, growths, tumor and holes in the ear drum. Identify the various parts of the eardrum and determine if it is normal.
Otoscopic Evaluation: This test is simply to check the ear canal. We evaluate the ear canal, structures of the ear canal and look for abnormalities (tumors, growths, etc.), wax, fluid, excessive ear hair, we assess the anatomy of the ear canal (narrow, closed, etc.), and evaluate the status of the eardrum. We look at the eardrum color, (red, white, yellow) the translucency (transparent, opaque) and position (retracted, neutral or bulging) of the drum. Look for scarring of the eardrum, growths, tumor and holes in the ear drum. Identify the various parts of the eardrum and determine if it is normal.
In our office we have a video otoscope where the patient can also look at his own ear canal and see what the Audiologist sees.
A Normal status of the Auditory canal: Some hair, often with yellow to brown mild cerumen.
Ear drum: a normal eardrum should be Pinkish gray in color, translucent and in neutral position.
We look at the status of one of the bones in the middle ear called the Malleus, we make sure that it lies in oblique position behind the upper part of the drum.
It's crucial that the ears are cleared of excessive wax otherwise this would interfere with accurate test results. WE DO NOT TEST IF EAR CANALS HAVE EXCESSIVE WAX OR THE EAR CANAL IS OCCLUDED WITH WAX.
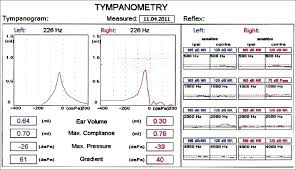
Tympanometric Testing: This examination is used to test the condition of the middle ear (found behind the eardrum) and mobility of the eardrum (tympanic membrane) and the conduction bones by creating variations of air pressure in the ear canal. Tympanometry is an objective test of middle-ear function.
This test is critical because abnormal readings require a medical referral. Patients will complain of sound being muffled, some ringing in the ears, ear pressure, fullness in the ears, the patient may hear popping sounds, etc. In abnormal cases where we see restricted mobility of the eardrum, the patient may have problems hearing because the sound is not being delivered properly to the middle ear. Most of the patients that have an abnormal reading of a non-mobile eardrum have a conductive or mixed hearing loss. This condition may need medical attention so it’s crucial that prior to considering hearing aids, the patient has a comprehensive hearing test.
 Acoustic reflex testing (ART):
Acoustic reflex testing (ART):
We have two muscles that are found in the middle ear, one called the stapedius muscle and the other one called the tensor tympani muscle. These muscles contract to high-intensity sound stimulus or when we vocalize. When these two muscles contract, they protect our ears from allowing loud sounds to come in.
The Acoustic reflex test:
With this test, we trigger the acoustic reflex. Individuals with normal hearing have an acoustic reflex threshold (ART) around 70-100 dB SPL. People with conductive hearing loss (-i.e. bad transmission in the middle ear) have a higher acoustic reflex threshold and those with severe hearing loss may have absent acoustic reflexes.
We also do more comprehensive testing such as ipsilateral (same side) and contralateral (opposite side) acoustic reflexes:
These tests will let us know if cochlear, vestibular, facial nerve, middle ear, intra-axial brainstem or extra-axial brainstem pathology might exist. (will show if there’s anything wrong)
An audiologist is familiar with the anatomy and physiology associated with the ART including the outer, middle, and inner ear structures, the vestibulocochlear nerve (VIII cranial nerve), and structures in the central auditory nervous system (CANS); specifically, auditory structures located at the level of the lower brainstem including the cochlear nuclei, superior olivary complex and facial nerve (VII nerve) nuclei.
 Tone decay test: It evaluates defects in adaptation to sounds, formally known as auditory fatigue–tone decay, which indicates a defect in retro cochlear (behind the cochlea, denoting the eighth cranial nerve and cerebellopontine angle as opposed to the cochlea) transmission of nerve impulses from the ear, possibly caused by pressure or 8th cranial nerve damage.
Tone decay test: It evaluates defects in adaptation to sounds, formally known as auditory fatigue–tone decay, which indicates a defect in retro cochlear (behind the cochlea, denoting the eighth cranial nerve and cerebellopontine angle as opposed to the cochlea) transmission of nerve impulses from the ear, possibly caused by pressure or 8th cranial nerve damage.
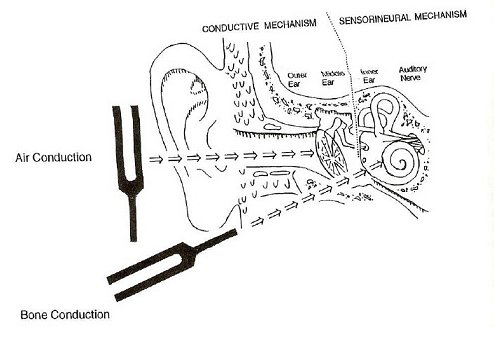
Air conduction testing: Determines if hearing loss exists. This is just a screening test, it does not let the provider know if a medical problem is present. Some dealers use just this test to fit hearing aids without doing a comprehensive hearing test.
Bone conductive testing with possible masking: Determines the type of hearing loss. Let’s the provider know if the patient would need a medical referral to a specialist (ENT).
 Bone conduction testing can indicate 3 types of hearing loss
Bone conduction testing can indicate 3 types of hearing loss
- Conductive hearing loss: This problem is with the sound being blocked in the ear canal or a medical problem behind the eardrum. Sometimes it is just wax in the ear that needs to be removed prior to testing (WE do not test patients who have wax in their ears; it must be removed prior to the comprehensive hearing test). Conductive hearing loss may be due to an ear infection, problems with one of the smallest bones in the middle ear (calcification known as Otosclerosis, or a broken or loose bone behind the eardrum, known as “Ossicular discontinuity”, pressure in the middle ear etc., this type of hearing requires a referral to a medical doctor. We do not discuss hearing aid options if we find any kind of medical red flag. The patient is to obtain medical clearance prior to hearing aid evaluation.
- Sensorineural hearing loss: This is permanent hearing loss that requires hearing aids. This problem comes from the inner ear known as the cochlea and associated structures such as the 8th cranial nerve.
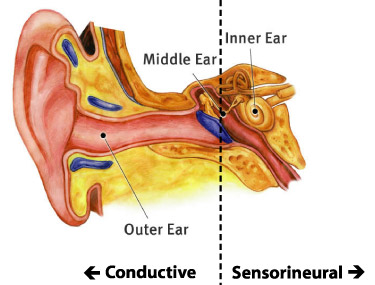
- Mixed hearing loss: This can be a combination of the above hearing losses. Reason why we work closely with ENT doctors to make sure that if a patient needs medical attention at any given time, that patient will receive the adequate help.
 Speech Reception Threshold test:
Speech Reception Threshold test:
Allows the clinician to find where the patient barely detects speech to use it as a cross check with the pure tone results (air conduction testing) obtained to determine the reliability of test results.
Speech Discrimination:
Test that provides the clinician with a percentage of correct words (decibel level used to present words above patients hearing loss and at a comfortable level). Use to provide the patient with an idea about how a patient might understand speech with a hearing aid in a quiet place “to provide patient with realistic expectations”. The longer the patient waits to get fitting with hearing aids, the more difficulty they will have in the future to understand speech.

Speech in Noise test: This is to inform the patient about how much he struggles understanding others in a noisy environment.
UCL: Most uncomfortable levels are tested to make sure that when hearing aids are programmed they don’t reach this level.
When in need, we perform tinnitus matching pitch test, for those whose suffer from ringing in the ears. We also provide with solutions for these patients and give them options.
Otoacoustic Emission test (OAEs): Is a sound which is generated from within the inner ear. Studies have shown that OAEs disappear after the inner ear has been damaged. OAEs are often used as a measure of inner ear health. OAEs are the basis of a non-invasive test for differential diagnosis of cochlear and higher level hearing losses (e.g., auditory neuropathy and even to identify a hidden hearing loss).
Auditory Brainstem Response (ABR): Is a recording of vertex positive waves of which I-V waves are evaluated. The ABR is used for determining pathologies beyond the cochlea to assess auditory nerve and brainstem function.
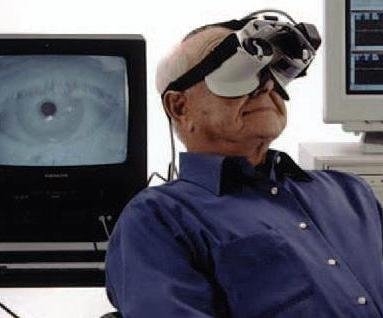 Videonystagmography (VNG): Involves the use of infrared goggles to track eye movements during visual stimulation and positional changes. VNG can determine whether dizziness is caused by inner ear disease as opposed to a central nervous system pathology.
Videonystagmography (VNG): Involves the use of infrared goggles to track eye movements during visual stimulation and positional changes. VNG can determine whether dizziness is caused by inner ear disease as opposed to a central nervous system pathology.
When a patient comes to an Audiologist office, our main concern is: is there anything medical going on in the ears that can be medically treated prior to use of hearing aids? Yes, we want to help people hear better and hence the recommendation of hearing aids but we are also concern about the medical aspect of our patients.
We offer all of the above tests in our Pasadena office and in our Rancho Cucamonga office as well but we also offer ABR and Vestibular testing in our Rancho Cucamonga office. If a patient needs an ABR or vestibular testing, they can visit our Rancho Office.